
Binge drinking of alcohol can lead to fatal consequences like alcohol ketoacidosis.
A 64-year-old-female presented tot the emergency department with complaints of diffuse abdominal pain, shortness of breath, nausea, and vomiting.
Blood was withdrawn for serological investigations. The arterial blood gases showed the following results, which revealed acidemia:
- pH of 7.10
- Bicarbonate of 2.9 mmol/l
- Lactate of 11.7 mmol/l
- The anion gap was calculated and was elevated at 25 mmol/l.
Other blood reports revealed raised serum ketones of 5.5 mmol/l. Capillary blood glucose was recorded to be 5.8 mmol/l.
A working diagnosis of diabetic ketoacidosis was made.
Soon after the diagnosis, a senior medical review was made to reassess the diagnosis. After a thorough history, it was revealed that the patient had a recent history of excess alcohol intake a day before presenting due to which a working diagnosis of alcoholic ketoacidosis was made.
With this working diagnosis, the patient was expected to have a decreased level of consciousness, but on the contrary, the patient was coherent enough to narrate her alcohol drinking habits. She reported drinking 1 to 2 bottles of wine per day for the past 30 years.
A multidisciplinary team was assigned to manage the patient, including the emergency physicians, the gastroenterologists, nurses, dietitians, alcohol specialist nurses, physiotherapists, and occupational therapists.
The patient was started on fluids, nutritional supplements, alcohol detoxification regimen, and she was monitored. The serological results improved with a substantial decrease in the level of ketones and normalization of pH. Following the resuscitation, the plasma electrolyte levels improved.
Given the prompt diagnosis of alcohol ketoacidosis and timely management, the patient showed substantial improvement. She was discharged, and she maintained her health during subsequent follow-up appointments.
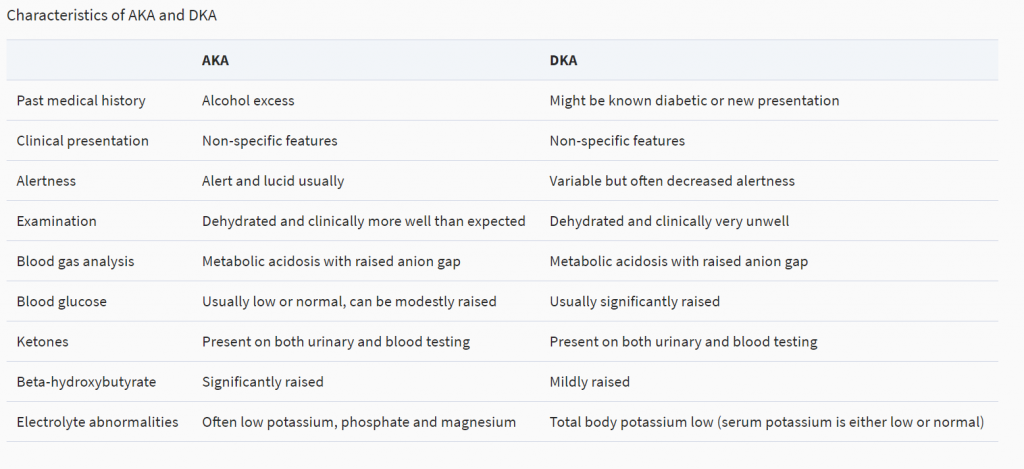
Any patient with severe metabolic acidosis and a recent history of binge drinking, chronic alcohol intake, or malnourishment should be evaluated for alcoholic acidosis. Due to the rarity, the diagnosis is often missed or delayed, leading to fatal consequences. One of the important differentials to rule out is diabetic ketoacidosis. The serological markers may overlap, but there are distinct clinical manifestations that help in differentiating DKA and AKA.
Fluid resuscitation and correction of electrolyte abnormalities remain the mainstay of treatment. It is imperative to diagnose accurately and treat promptly to avoid any fatal complications, including cardiac arrhythmias, which may occur secondary to electrolyte abnormalities.


