- Necrotizing Fasciitis is an infection of the deep soft tissues, including muscle fascia and fat.
- Its risk factors include trauma, malnutrition, diabetes mellitus, neutropenia, alcoholism, and cirrhosis
- Clinically, the disease picture includes fever, pain, erythema, crepitus, and skin abscesses
- It is a rare occurrence, with an incidence rate ranging from 0.3 to 15 cases per 100,000
This report describes the case of a 58 year old female cancer patient who suffered from necrotizing fasciitis due to her chemotherapy medication.
Medical History
The middle aged female patient had a medical history of hypertension and controlled diabetes mellitus. In 2013, she was diagnosed with stage VI ovarian clear cell carcinoma which also involved her abdominal lymph nodes. She was treated for the cancer with an abdominal hysterectomy and bilateral salpingo-oophorectomy in the same year. The patient was then prescribed chemotherapy cycles to further improve her prognosis. However, in 2019, the patient presented with a complaint of week-long rectal bleeding. Upon screening, the doctors confirmed that her tumor had returned and had metastasized into her sigmoid colon. They performed a partial colectomy to remove the tumor and prescribed adjuvant chemotherapy, which she did not receive for a year.
Upon return, the patient underwent a chemotherapy regimen consisting of bevacizumab, paclitaxel, and carboplatin. 5 months into this regimen, she presented to the emergency department complaining of pain and swelling in her right gluteal region for a week, along with fever and chills. The pain did not radiate, and her bowel or urinary habits had not changed.
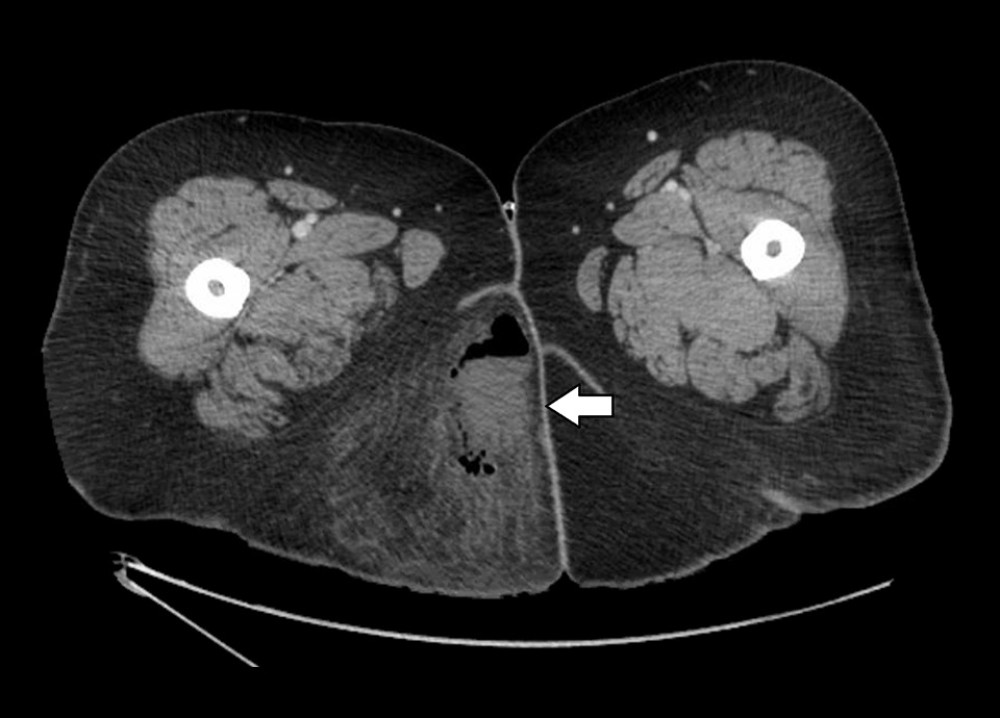
A general examination revealed a heart rate of 135 bpm, blood pressure 142/77 mmHg, 38°C temperature, and 96% oxygen saturation. Upon visual examination of her right gluteus, the doctors found a fluctuant indurated mass. The abscess did not have a drainage site, and did not mar the skin. Blood tests revealed elevated neutrophil count (83%) and C-reactive protein presence, with lactic acidosis. Furthermore, a contrasted computerized tomography (CT) scan confirmed the presence of an air-fluid abscess measuring 7.4×4.1 cm in size.
The doctors diagnosed this patient with necrotizing fasciitis based on this clinical and pathological picture.
Necrotizing Fasciitis
Necrotizing fasciitis is an infective disease that damages the deep muscle fascia and fat. Symptoms include fever, pain, erythema, and skin abscesses. There are many risk factors for this disease, including trauma, obesity, uncontrolled diabetes mellitus, alcoholism, and recent surgery.
According to the case report, however, the authors relate the occurrence to the patient’s use of the chemotherapeutic drug bevacizumab. She was taking this drug for her cancer reoccurrence and was on it for 5 months.
The drug is a human monoclonal IgG antibody, used to treat metastatic ovarian cancers. It acts as a vascular endothelial growth factor (VEGF) inhibitor and is used as chemotherapy to counteract the angiogenesis caused by tumors. This occurs due to the tumor’s growing need for oxygen to support its growth and metabolism. Inhibiting the vascular growth cuts off the tumor’s oxygen supply, forcing its growth to slow down.
However, previous studies have shown that bevacizumab can cause thromboembolism. This effect, combined with its antiangiogenic properties, may cause tissue ischemia and necrosis. The drug is also associated with poor wound healing, creating an ideal environment for bacteria to grow and flourish.
This aspect of the drug’s safety was demonstrated through a 15 year study which reported that 52 trial subjects suffered from necrotizing fasciitis while on bevacizumab.
Rationale
The authors of the case report state:
“It is difficult to establish a causal relationship between bevacizumab and necrotizing fasciitis in patients receiving chemotherapy who are already immunocompromised. However, since these patients are already immunosuppressed, it becomes even more important to explore this association…”
They continue to explain that while diabetes mellitus is also a causative factor that affects immunity, the patient’s diabetes was well controlled with a hemoglobin A1c level of 6.6% (threshold is <8%) and did not show any vascular extension. She also did not have history of trauma or ulceration, two other risk factors associated with necrotizing fasciitis.
Therefore, the doctors suspected that bevacizumab was the core cause of this event.
Treatment
According to the literature, adverse events warrant a temporary discontinuation of bevacizumab depending on the patient’s condition. However, the drug must be permanently discontinued following events like hemorrhage, thromboembolism, gastric perforation, or necrotizing fasciitis.
While the diagnostic testing was underway, the patient suffered from an event of septic shock. The clinical team administered low-dose norepinephrine for this. They proceeded to treat the abscess through incision and debridement and drained off 200ml of foul-smelling pus from it. Initially, they began a prophylactic regimen of IV broad spectrum antibiotics. These were stopped in favor of only ciprofloxacin after the sample culture from the abscess returned positive for Escherichia Coli (E. coli). The blood sample culture however, was negative. The doctors also tapered the norepinephrine off, discharging the patient with outpatient follow-up advised.
Reference:
Haider, A., Gurjar, H., Ghazanfar, H., & Chilimuri, S. (2022). Necrotizing Fasciitis In A Patient with Metastatic Clear Cell Ovarian Carcinoma Treated with Bevacizumab. The American journal of case reports, 23, e935584. https://doi.org/10.12659/AJCR.935584


