A rare case of a dermoid cyst with an atypical appearance
Intracranial dermoid cyst is rare benign tumour that typically exhibits classic computed tomography (CT) and magnetic resonance imaging (MRI) characteristics, making diagnosis relatively simple. Because of their diverse ectodermal-derived content, atypical imaging features can occur, resulting in a diagnostic quandary. Making an accurate diagnosis is critical for proper management.
Dermoid cysts account for less than 1% of all primary intracranial tumours. They are benign congenital inclusion cysts that develop from ectodermal tissue during embryogenesis. The most common locations are the midline sellar, parasellar, frontonasal, and posterior fossa. Their imaging appearance may vary due to their diverse ectodermal-derived content, which includes apocrine glands, sebaceous glands, hair follicles, and/or teeth. Almost all dermoid cysts, however, exhibit classic lipid-containing characteristics, such as a hypodense appearance on CT, hyperintensity on T1-WI with no contrast enhancement, and a heterogeneous signal intensity on T2-WI. A case of an intracranial dermoid cyst with unusual imaging features is presented.
Case study: intracranial dermoid cyst
A 39-year-old woman with a history of high blood pressure was referred to a healthcare facility after a head computed tomography (CT) performed at another hospital revealed a possible posterior fossa hematoma. Further history revealed a 6-month onset of headaches with recent worsening and non-resistance to NSAIDs. The patient denied experiencing nausea, vomiting, vision changes, or fever. There was no mention of any recent trauma. There were no neurologic deficits revealed during the physical examination.
Investigation findings
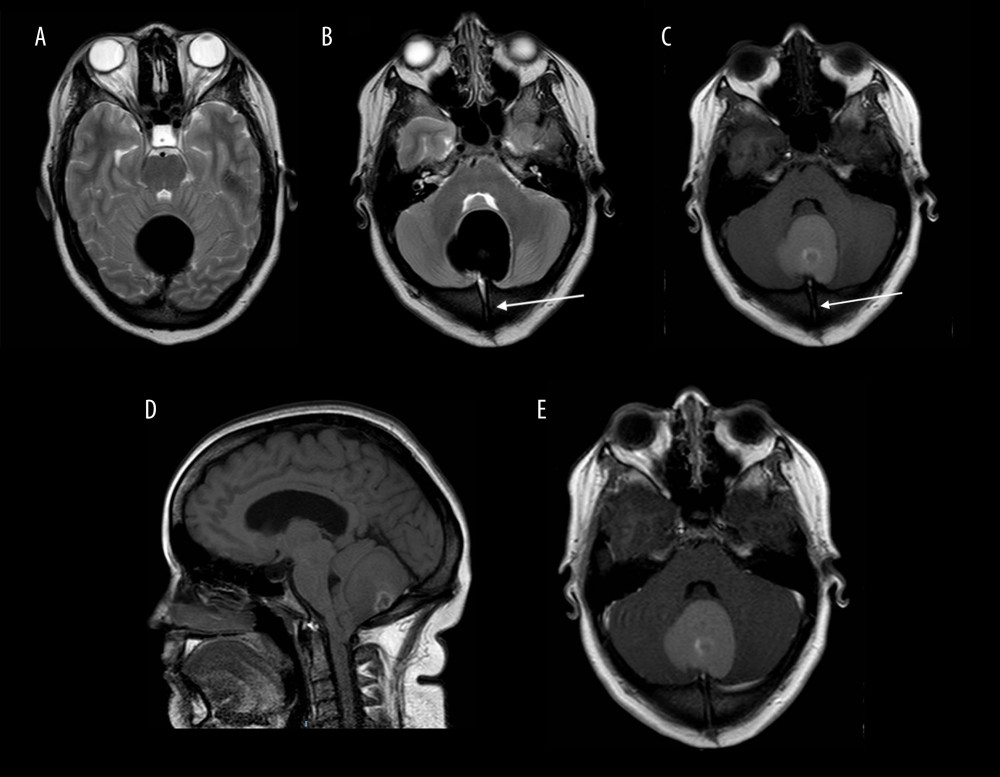
The MRI revealed a well-defined T1 hyperintense and T2 profoundly hypointense extra-axial lesion in the midline posterior fossa, with susceptibility artefact, no restricted diffusion, and no contrast enhancement, measuring 4.0 cm transverse by 3.8 cm AP by 4.9 cm CC. The lesion caused a local mass effect on nearby structures, resulting in partial compression of the vermis and bilateral cerebellar hemispheres, as well as tonsillar herniation. Mild supratentorial obstructive hydrocephalus was caused by partial compression of the fourth ventricle and fourth ventricular outflow tract. MRI revealed a transdiploic linear channel.
There was also a partially empty sella and bilateral optic nerve disc flattening, as seen with increased intracranial pressure. The lesion was found to have homogenous hyperdensity on a non-contrast CT scan (Figure 2), with better delineation of the overlying midline occipital transdiploic channel. A profoundly hypodense focus within the transdiploic channel near the lesion measured 13 Hounsfield units and, based on its increased signal intensity on MRI, could represent a small fat focus. The occipital bone appeared to have mild relative thickening. To rule out a vascular cause, catheter angiography was performed (Figure 3), which revealed no evidence of a vascular lesion or neoplastic/tumoral blush.
Diagnosis and treatment
With a preoperative diagnosis of a posterior fossa brain mass, the patient underwent suboccipital craniotomy for lesion resection. Cholesterol clefts and hair shafts, as well as luminal lamellated keratin flakes, were discovered during the histopathologic examination. Foreign-body type (multinucleated) giant cell reactions and pigment-laden macrophages were also discovered. These findings are consistent with the presence of a dermoid cyst. The patient showed full recovery after treatment.
Dermoid cysts are intracranial tumours with distinct imaging characteristics. We present a case of an intracranial dermoid cyst, a rare intracranial tumour with atypical imaging characteristics on CT and MRI. Understanding these unusual radiologic features is therefore critical in the imaging analysis of these lesions. In conclusion, Most dermoid cysts are treated with complete surgical resection. Atypical radiologic features in an intracranial tumour, which is already rare, can delay proper diagnosis and management. Recognizing these findings is thus critical for accurate imaging analysis of these lesions.
Source: American Journal of Case Reports


