This article describes the case of relapsing polychondritis in a 58-year-old patient with a history of human immunodeficiency virus (HIV) infection and chronic reactive arthritis. The patient presented to the emergency department with severe acute left eye pain, redness and swelling with a history of 2 weeks. Other symptoms included blurred vision, photophobia, and watery discharge. However, there were no signs of itching or vision loss.
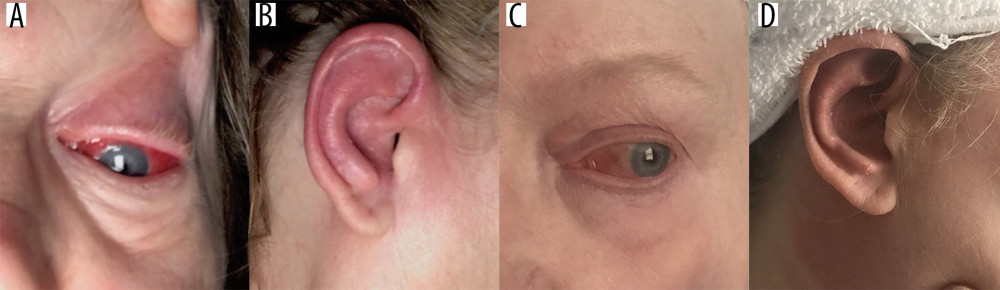
The patient was referred to ophthalmology where she was diagnosed with left eye scleritis and corneal ulceration. She also complained of right ear burning pain, redness and swelling. However, in the absence of discharge, tinnitus, hearing loss, loss of appetite or arthralgia. Moreover, there were no signs of urinary symptoms, change in bowel habits, weight change, joint swelling, rash, oral ulcers, fever, change in voice, cough or shortness of breath.
The patient’s medical history was revealed HIV controlled on HAART and a 12-year history of chronic reactive arthritis
She also had a family history of an unknown malignancy in her father. In addition, she was a former smoker and denied the use of alcohol or drugs. On presentation, the patient was afebrile with stable vital signs. She was breathing comfortably and had an oxygen saturation of 95% on ambient room air. Physical examination was consistent with right auricular erythema, swelling and tenderness with no ear discharge. Similarly, other findings included left scleral redness, mild left eyelid erythema and swelling with clear water discharge. However, there was no change in vision. Chest and musculoskeletal examinations were unremarkable.
Blood work was unremarkable. Infectious diseases including syphilis, tuberculosis, and Lyme disease were also ruled out. Based on the findings of left eye idiopathic orbital inflammation, scleritis, and right auricular chondritis, doctors diagnosed the patient with relapsing polychondritis.
Relapsing polychondritis
Relapsing polychondritis is a rare autoimmune condition that affects cartilaginous structures, the ears, nose, respiratory tract and joints. Although the aetiology of the disease is unknown, it is often associated with other systemic autoimmune diseases, malignancies and sometimes human immunodeficiency virus (HIV) infection. Doctors initially treated the patient with antibiotics. There was no clinical improvement. After excluding diagnostic possibilities and diagnosis of relapsing polychondritis, the patient was treated with corticosteroids and immunosuppression therapy. The patient showed significant clinical improvement and the corticosteroids were tapered off.
Source: American Journal of Case Reports


