Synthethic cannabinoid-induced (K2) posterior reversible encephalopathy syndrome (PRES)
K2 is a term used for artificially engineered cannabinoids that are often misused as psychedelic agents. According to a study conducted on college students in 2016, 7.6% of the students at college entry prevalently used cannabinoids. Over the years, synthetic cannabinoids have gained significant popularity because they are cheaper and aren’t easily detected on standard drug screenings. It is commonly used among low-income individuals, especially high school and college students. This is often linked with posterior reversible encephalopathy syndrome (PRES).
K2 can either be smoked using E-cigarettes, joints or pipes. Moreover, it can also be brewed as a tea. While SCBs are often similar in mechanism to natural marijuana, it is known to cause greater toxicity compared to natural marijuana. The majority of K2’s systemic effects come from its complete agonist action on CB1R and CB2R. While CB2Rs are concentrated in the hippocampus and ventral tegmental area and control the dopaminergic pathway, CB1Rs are widely distributed throughout the brain. The stimulation of CB receptors, which results in an abrupt reduction of synaptic neurotransmitter release in the brain, is one of the hypothesised mechanisms of PRES caused by K2 ingestion. Patients with K2 toxicity may also exhibit aggressive behaviour, hallucinations, paranoia, anxiety attacks, nausea, headache, chest pain, tachycardia, difficulty speaking, memory loss, numbness, seizures, stroke, and hallucinations. K2 toxicity can, in extreme circumstances, result in cardiac arrest and abrupt liver failure.
In this article, we describe a young, healthy patient who, after ingesting K2, acquired posterior reversible encephalopathy syndrome (PRES) despite having no known comorbidities.
Case study
The patient is a 24-year-old woman who had been acting abnormally at home. She was brought by emergency medical services to the emergency room. According to her mother, she discovered her daughter awake at around 1:00 a.m. “crying, clenching her teeth, and screaming incomprehensibly”. She claimed that for the previous three days, her daughter had also been suffering from intermittent, non-specific headaches. Her previous medical histories were unremarkable. There was no notable family history of autoimmune, neurologic or psychiatric disorders.
She was evaluated in the Emergency Department and was found to have episodic agitation, with bouts of crying followed by blank staring. The patient had a pulse rate of 98 beats per minute, a temperature of 37.1°C, a respiratory rate of 18 breaths per minute, a blood pressure of 114/76, and was saturating 98% on room air. Physical examination revealed that the patient was anxious and drowsy. Similarly, she was only oriented to place, but she could follow simple commands. Upon lung auscultation, she had bilateral vesicular breathing. A cardiac examination revealed normal S1 and S2 heart sounds. The abdominal and neurological exams were unremarkable.
Investigations and findings
An initial computed tomography (CT) head revealed no signs of acute pathology, and a chest X-ray and CT of the abdomen and pelvis were normal. The results of the complete blood count, electrolytes, creatinine, liver function test, creatine kinase, and ammonia blood tests were all normal. Positive nitrites, leukocyte esterase, and bacteria were found in the urine. Cannabinoids were detected in her urine drug test.
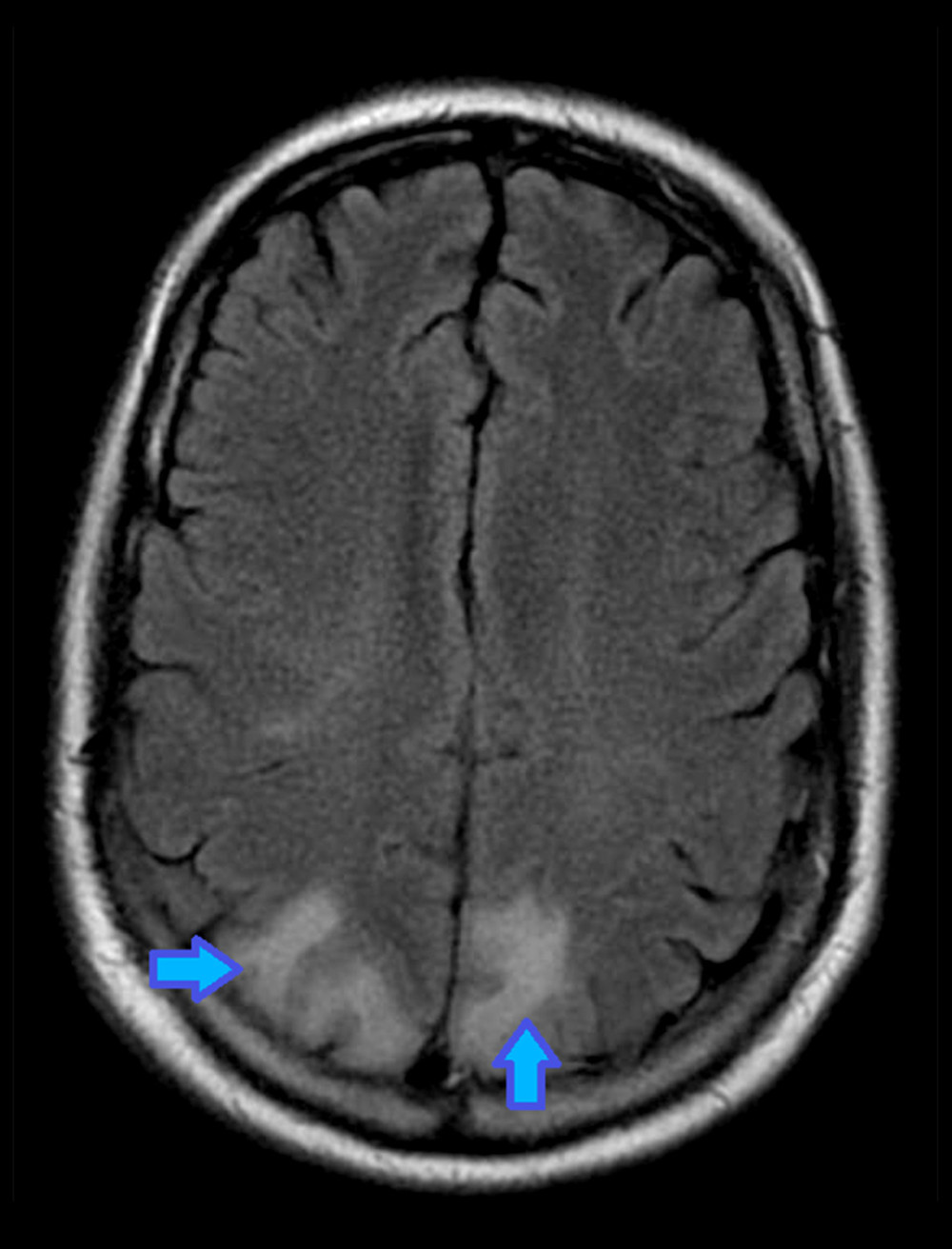
For a possible urinary tract infection, she was started on ceftriaxone and admitted to the inpatient service for further evaluation. On the fourth day of her hospitalisation, she became increasingly agitated and was determined to be a danger to herself and others. In addition, haloperidol was administered as needed to treat delirium and agitation. She had an electroencephalogram, which revealed bilateral slowing and disorganisation of background rhythms, indicating diffuse encephalopathy. Doctors further referred her for an MRI which revealed no haemorrhage, masses, or recent infarcts. High T2/FLAIR signal intensities were observed in the parietal cortices, the findings were significant with the diagnosis of PRES.
Given the MRI findings, the acute onset of neurocognitive symptoms such as headaches, seizures, confusion, nausea, and vomiting, and a history of cannabinoid use, the diagnosis of posterior reversible encephalopathy syndrome was made in the absence of clinical evidence of an infectious or autoimmune process. She was kept on levetiracetam for seizure prevention and olanzapine for agitation as needed. Her extensive drug screen revealed a positive result for K2. After three weeks in the hospital, her clinical condition improved, and she was discharged home with outpatient neurology follow-up.
She reported feeling well three months after discharge and was preparing to return to work. She also stated that she no longer used marijuana or K2.
Source: American Journal of Case Reports


