
Since its emergence in December 2019, the SARS-COV-2 (severe acute respiratory syndrome coronavirus 2) virus has managed to infect more than 1.8 million people worldwide and cause 117,000 deaths so far. Common symptoms of COVID-19 seem to be cough, fever and difficulty breathing. However, as the infection spreads globally, doctors are discovering more and more symptoms of this viral infection that were never before thought to be associated with coronaviruses. Thus, leading researchers to believe that the novel coronavirus might not just be limited to the respiratory tract.
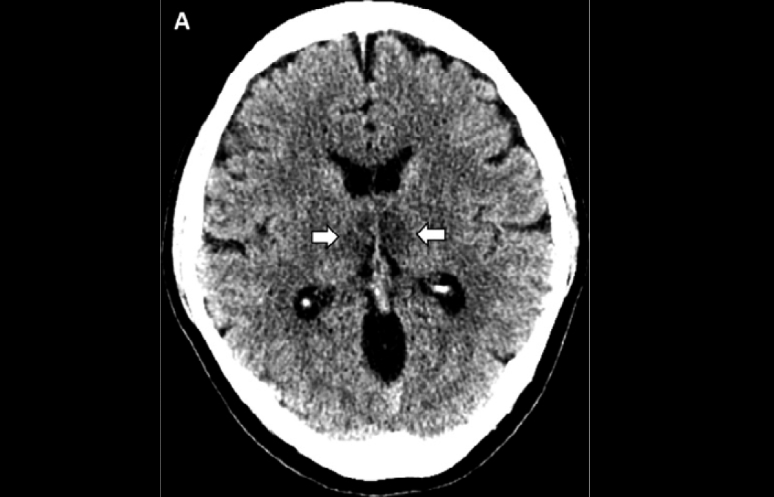
A 58-year-old airline worker recently became the first known case of a person developing acute necrotizing encephalitis (ANE) due to COVID-19. She had presented to the hospital with fever, cough and an altered mental state. The doctors at Henry Ford Health System, Detroit, conducted multiple tests to rule out influenza, Herpes, West Nile Virus, a bacterial infection of the cerebrospinal fluid (CSF) and, found her to be COVID-19 positive. According to Dr. Elissa Fory, “The team had suspected encephalitis at the outset, but then back-to-back CT and MRI scans made the diagnosis“.
According to a study published in the Journal of Medical Virology, patients with COVID-19 may also show other signs such as headache, nausea, vomiting, suggesting that the infection may also be affecting the neurological system. Recently there have also been numerous reports of COVID-19 patients complaining of loss of smell and taste, headaches and lethargy along with the usual fever and cough. It is believed that 10-15% of post-viral anosmia cases are thought to be due to coronaviruses. A case report published in the journal JAMA otolaryngology details the case of a 40-year-old woman, COVID-19 positive, who presented with a sudden and complete loss of smell without any nasal obstruction. She also complained of a cough, headache and muscle pain. CT scan of the nasal cavity showed bilateral inflammatory obstruction of the olfactory clefts without any obstruction and no history of rhinorrhea.
Coronaviruses can invade the brain
Previous studies had shown SARS-COV (severe acute respiratory syndrome coronavirus) to have the ability to enter the brain via the olfactory bulb, resulting in rapid, trans-neuronal spread to connected areas of the brain. SARS-COV was responsible for the SARS (Severe Acute Respiratory Syndrome) outbreak of early 2000s, which affected more than 8000 people worldwide. The study found that the virus would cause death by causing dysfunction and/or death of the infected neurons especially of those located in cardiorespiratory centers in the medulla.
A recent study published in JAMA Neurology looked at 214 patients with COVID-19. 36.4% of the patients were seen to have neurologic symptoms, more so if the patient had a severe infection. They concluded that these neurological symptoms can exist also in the absence of the typical COVID-19 symptoms such as fever, cough, diarrhea.
Although research points to the fact that coronaviruses can invade the brain and cause neurological symptoms, it is still unclear whether these signs and symptoms are due to direct infection of the nervous system cells or if underlying conditions can be triggered via the infection.
References:
Mao L, Jin H, Wang M, et al. Neurologic Manifestations of Hospitalized Patients With Coronavirus Disease 2019 in Wuhan, China. JAMA Neurol. Published online April 10, 2020
Netland, J., Meyerholz, D. K., Moore, S., Cassell, M., & Perlman, S. (2008). Severe acute respiratory syndrome coronavirus infection causes neuronal death in the absence of encephalitis in mice transgenic for human ACE2. Journal of virology, 82(15), 7264–7275. https://doi.org/10.1128/JVI.00737-08
Eliezer M, Hautefort C, Hamel A, et al. Sudden and Complete Olfactory Loss Function as a Possible Symptom of COVID-19. JAMA Otolaryngol Head Neck Surg. Published online April 08, 2020.
Li, Y‐C, Bai, W‐Z, Hashikawa, T. The neuroinvasive potential of SARS‐CoV2 may play a role in the respiratory failure of COVID‐19 patients. J Med Virol. 2020; 1– 4.


