Case of focal seizures in a school-aged boy during adrenocorticotropic hormone therapy
It has been reported that adrenocorticotropic hormone (ACTH) therapy for infantile spasms, including West syndrome, can cause seizures. These ACTH-induced seizures are defined as new seizures that occur during ACTH therapy and disappear once ACTH therapy is stopped. ACTH-induced seizures, on the other hand, have not been described in patients with focal seizures other than epileptic spasms, patients without a history of epileptic spasms, or patients older than one year.
Case presentation: focal seizures
This article describes the case of an ACTH-induced seizure in a school-aged child. The findings, in this case, show that ACTH-induced seizures can occur in older patients suffering from intractable seizures other than epileptic spasms. The patient in this case study is a 14-year-old Japanese boy who suffered a traumatic brain injury in a car accident when he was 6 years old. This injury caused partial damage to the right frontoparietal lobe and left frontal lobe, as well as right enophthalmos, left hemiplegia, and loss of vision in the right eye.
At the age of ten, he became unconscious after having generalised seizures and was diagnosed with secondary generalised tonic-clonic seizures. Treatment with levetiracetam, sodium valproate, lamotrigine, clobazam, zonisamide, perampanel, phenobarbital, clonazepam, or lacosamide did not stop his seizures. Seizures were recorded on a monthly basis. When carbamazepine was administered to a 13-year-old boy, he experienced brief muscle contractions of the upper limb, and these seizures persisted after the carbamazepine was stopped.
Investigations and findings
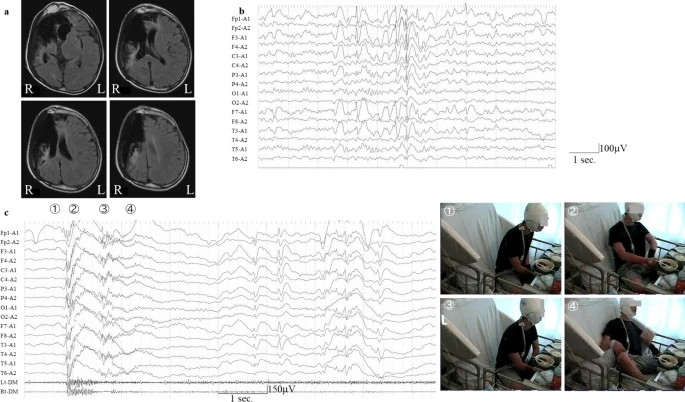
Interictal electroencephalography (EEG) revealed high-amplitude spikes or spikes and waves in the frontal region from the left frontal pole to the frontal region. The ictal EEG revealed generalised rhythmic spike bursts preceded by a spike wave in the left hemisphere, followed by slow-wave bursts with left hemisphere dominance corresponding to his habitual seizures, which were characterised by turning his head to the left and left upper limb flexion along with muscle contraction in a sitting position after a 5-second fall backwards and unawareness.
The seizures were diagnosed as focal seizures. In addition to the previously mentioned medications, oral administration of rufinamide and clorazepate had no effect on seizure frequency. At 10 months after video EEG monitoring, ACTH therapy (synthetic ACTH, a zinc hydroxide suspension of tetracosactide acetate; Cortrosyn-Z [Daiichi-Sankyo, Japan]) was started after obtaining informed consent. ACTH was given as daily intramuscular injections (0.0125 mg/kg) for two weeks before being gradually tapered off over one week. On day 10 of ACTH therapy, he developed new focal seizures characterised by left arm contractions followed by movements of touching things with his right hand and writhing and rocking his body left and right and back and forth as automatisms, despite the fact that his previous seizures had vanished transiently.
The ictal EEG of newly developing focal seizures showed generalised low-voltage fast waves followed by high voltage in the left hemisphere only, which was then followed by high-voltage slow-wave bursts with left hemisphere dominance on video EEG monitoring. The focal seizures lasted 40 minutes and were relieved by suppository administration of 10 mg diazepam. Interictal EEG 4 days after the onset of the new seizures revealed spikes in the left frontal region.
Prognosis
After more than two years of monitoring, these focal seizures did not reoccur. After the onset of focal seizures, no new lesions were found on brain computed tomography. His habitual seizures prior to ACTH therapy vanished briefly on day 10 of therapy; however, they reappeared on day 14 after ACTH therapy.


