Emphysematous aortitis
Emphysematous aortitis is a rare condition that is characterised by the presence of air either within or surrounding an inflamed aorta. Aortic inflammation may occur because of an infective or non-infective cause. In addition, timely diagnosis and treatment of this rare disease are important to prevent clinical deterioration that may lead to inevitable death. Studies have shown that cross-sectional imaging is an important tool for the diagnosis and management of infectious emphysematous aortitis. In addition, other than its contribution to diagnosis, it is also widely available. This article describes the case of a 74-year-old with a history of end-stage kidney disease and coronary artery disease diagnosed with infectious emphysematous aortitis.
Case report
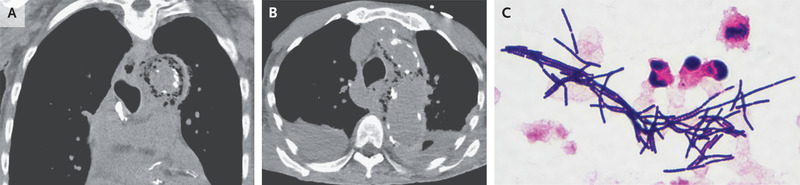
A 74-year-old male patient was brought to the emergency department for decreased responsiveness during haemodialysis, with a 3-day history of anorexia and generalised weakness. Other symptoms included a 3-day history of anorexia and generalised weakness. The patient’s medical history was significant for end-stage kidney disease and coronary artery disease. On examination, the patient appeared ill and only responded briefly to the questions. For further evaluation, doctors advised a chest radiograph which showed a widened mediastinum. The patient was also referred for computed tomography without the administration of intravenous contrast material. The findings of the CT showed intramural gas in the ascending and descending aorta with signs of aortic calcification.
Anaerobic blood cultures showed the growth of gram-positive rod and Clostridium septicum. Based on these findings, the patient was diagnosed with infectious emphysematous aortitis. Studies have further shown that C. septicum infection increased the risk of gastrointestinal cancer. The organism supposedly enters the bloodstream through the gastrointestinal tract. However, in case of an endovascular infection, it may lead to atherosclerotic plaques as in this case.
The patient’s medical history further revealed that he was positive for Clostridum septicum on fecal immunohistochemical testing three years before this presentation. Doctors advised a colonoscopy, however, the patient declined. There were no signs of cancer on the abdominal imaging performed on the current hospitalisation. Although surgery is the treatment of choice for this type of infection, the patient was unfit for surgery. Therefore, he was treated with intravenous penicillin G and clindamycin. He died on the 7th day of hospitalisation while receiving comfort care [1].
Aortitis
Aortitis is defined as an inflammatory process that involves the aortic wall. It is either infective or non-infective in origin. Under normal conditions, the aorta is very resistant to infection. Although there are some conditions that may increase the risk of infection including, diabetes, preexisting aneurysms, atherosclerotic disease and other immune-susceptible states, for example, open surgery or the presence of medical devices.
A wide range of organisms can cause infectious emphysematous aortitis including Staphylococcus aureus, Salmonella, Pneumococcus, Escherichia coli, Treponema pallidum, Candida, Aspergillus and Tuberculosis. Prompt diagnosis is critical for the treatment of patients. The term “mycotic aneurysm” was first coined in 1885 by Osler, meaning mushroom-shaped infectious aneurysms associated with bacterial endocarditis. In addition, the Salmonella spp is the most commonly identified causative agent of primary infection of aortic aneurysms. Similarly, the presence of Clostridium septicum have been linked with infective endocarditis and colonic malignancy.
Diagnostic challenges
The aorta is generally resistant to infection under normal circumstances. However, certain conditions may predispose it to infection, for example, an underlying aneurysm, atherosclerotic disease, presence of a medical device and patients who are immune-compromised. Cross-sectional imaging is an important tool for diagnosis and further management of the condition. Patients with infectious emphysematous aortitis are often systemically unwell, thus images with shorter acquisition time are preferred, for example, CT scans.
CT scan findings for aortitis are significant for vertebral body destruction, gas formation and air pockets, rapidly enlarging aneurysm, periaortic fluid and aortic wall thickening. Additionally, early signs of infection may include periaortic asymmetric fat stranding and the presence of a soft tissue mass. A more advanced stage of the disease is significant for the presence of periaortic gas and vessel wall emphysema. However, with the wide availability of antibiotics, most of these signs are usually not seen. Thus, accurate diagnosis remains a challenge for treating physicians, especially because of non-specific clinical signs and symptoms.
References
Traver, E.C. and Gao, N.J., 2022. Emphysematous Aortitis. New England Journal of Medicine, 386(19), pp.1833-1833.


