Colonic pseudolipomatosis, secondary to iatrogenic injury
Colonic pseudolipomatosis is a benign condition that can pose a diagnostic challenge because of its rarity. Similarly, because the condition is rare and most endoscopists are familiar with it, the diagnosis can be confused with other lesions. There have been a few reports where the patients were diagnosed with the condition by endoscopists.
The aetiology and pathogenesis of colonic pseudolipomatosis are not clarified completely. It can also be related to iatrogneic injury during an endoscopic examination. In addition, due to a chemical injury caused by residual disinfectants, after cleansing on the surface of the scope. Imaging tests including CT scan and MRI do not aid in diagnosis. However, the lesions can be differentiated from pre-malignant lesions with the characteristic endoscopic features. This article describes the case of an asymptomatic patient diagnosed with colonic pseudolipomatosis while undergoing screening for cancer.
Case report
In this case, a 65-year-old male patient from Rio de Janeiro presented with mild constipation that was under control with regular intake of fibre. The patient’s medical history did not reveal any comorbidities. All the endoscopies the patient underwent prior to 2018 did not show any polyps. However, the last exam done in 2018 showed a microvascular hyperplastic polyp that was retrieved from the sigmoid colon. The patient did not show any symptoms previously. However, because of a strong family history of colorectal cancer, he underwent a colonoscopy in 2021. Doctors advised a complete exam after bowel preparation.
Doctors biopsied the lesions. Findings showed that the colonic segments were unremarkable. Histopathological analysis showed an accumulation of gas in the colonic mucosa. In addition, the lamina propria showed clear air spaces of different sizes surrounded by an inflammatory infiltrate. Histopathology further showed that the air spaces were in aggregates, isolated and confluent with an empty centre. It was further composed of eosinophils and mononuclear cells. Giant multinuclear cells were absent.
The epithelial lining was slightly reactive and hyperplastic and maintained regular architectural organization in the absence of nuclear atypia. The air spaces were similar to fat cells, therefore, known as pseudolipomatosis. It was distinguished from adipose tissue because of its focal nature and lack of nuclei.
Discussion
Snover et al first coined the term pseudolopomatosis in 1985. CP is described as a rare benign condition that has a prevalence of 0.02% to 0.3%. It is more commonly diagnosed in individuals in their 50s and 60s. However, there is no clear sex prediliction. Generally patients are asymptomatic but in some cases, they may present with diarrhoea, lower GI tract bleeding, bloating and positive fecal occult blood test. The lesions generally disappear without any treatment over a few weeks. It is more commonly seen in the left colon but in some cases, the lesions may be right- and left-sided. The lesions are also seen in the rectum, skin, duodenum, stomach, endometrium and oral/nasal mucosa.
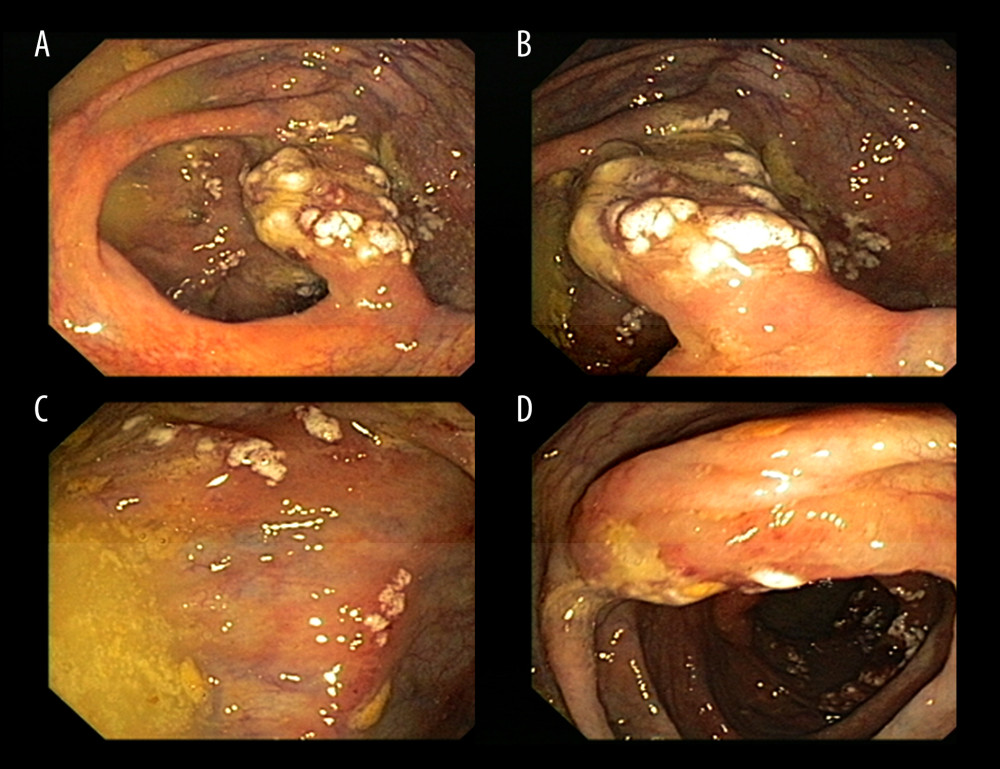
The lesions are yellow or whitish, single or multiple and sometimes appear as confluent plaques in 1 or more colonic segments. The size of the lesions varies from 0.2 to 5 cm in width, with peripheral erythema. The lesions are commonly visualised when the endoscope is being withdrawn. However, in some cases, the lesions may also be found during insertion. Staining for fat and mucin are generally negative. Whereas cholesterol crystals are also not visualized in the exam with polarized light.
Diagnosis
There are no signs of lipid deposits, and labs are usually negative for anti-CD 31, anti CD 34 and anti-protein S100. Differential diagnoses include colonic lipomatosis, cystic pneumatosis, colonic lymphangioma, hyperplastic lipomatosis, pseudomembranous colitis, malakoplakia and colonic lipomas. A demarcating feature is that unlike lipomatosis, there are no adipose cells in pseudolipomatosis. In cystic pneumatosis, the colonic epithelial lining presents with mild local oedema and gas bubbles that burst as the mucosal layer retracts. Histopathological analysis shows empty cysts in the submucosa, with macrophages and giant cells infiltrates surrounding the cysts.
While CP is not considered an infectious disease, the etiology and pathogensis are still unclear. The lesions can be related to either iatrogenic injury because of epithelial stretch, hyperinsuffiation, biopsy or abrasion. This allows the gas to infiltrate into the colonic wall. CP has also been linked with chemical injury because of residual disinfectants on the surface of the scope after it is cleaned with hydrogen peroxide.
Although a pulmonary source of gas is unlikely, experiments in animals and cadavers have rarely reproduced submucosal cysts. However, subserosal cysts are observed. A study by Snover and Cox suggests that the lesion may be operator-dependant. In conclusion, colonic pseudolipomatosis is a rare and benign condition that is often mistaken for serious conditions. Although, it does not require any treatment or further investigations. The key to avoid unnecessary procedures in a proper diagnosis, as with this case, also.
Source: American Journal of Case Reports


