15-year change of an adrenal endothelial cyst
Adrenal gland cysts are uncommon and frequently go undetected. Nonspecific symptoms, such as abdominal or flank pain, can occur if tumours grow large enough to compress nearby organs. Even with advanced imaging modalities, it is difficult to distinguish between benign and malignant adrenal neoplasms. As a result, determining a definitive diagnosis and providing treatment is challenging. We present the case of a 76-year-old man who was found to have a suspected cystic neoplasm of the adrenal gland after a 15-year follow-up period and underwent adrenalectomy.
Case study
A 76-year-old man presented with an asymptomatic adrenal incidentaloma (64 cm in size). He was diagnosed with a left adrenal lesion 15 years ago, according to his medical history. There were no obvious abnormalities, including cushingoid symptoms, on physical examination. A hypoechoic nodule in the left suprarenal region was discovered during the initial abdominal sonography. Abdominal computed tomography (CT) revealed a Hounsfield unit value of 40 and ring enhancement over the left adrenal gland; malignancy was suspected. A well-defined, round nodular lesion measuring 3.84 cm over the left suprarenal region was revealed by an abdominopelvic magnetic resonance image (MRI).
The central section had a relatively high signal but no significant contrast medium enhancement; the peripheral section, on the other hand, showed moderate contrast medium enhancement. When comparing out-of-phase images to in-phase images, the entire nodule did not decrease signal intensity. Abdominal ultrasound images revealed no discernible changes in the nodule during regular follow-up evaluations every 6 months for 8 years.
The patient did not follow up until 7 years later.
Investigation findings
There was no abdominal pain, discomfort, or palpable masses on the flank or abdominal wall. Laboratory data revealed mild hypokalemia (2.9 mmol/L), while the remaining blood tests and urinalysis results were all within normal limits. The patient did not receive any specific medication. A full endocrine evaluation was carried out, including measurements of urinary vanillylmandelic acid (3.5 mg/24 h), serum cortisol (8.39 ug/dL), plasma renin activity (0.56 ng/mL/h), aldosterone (133.9 pg/mL), and testosterone (201 ng/dL).
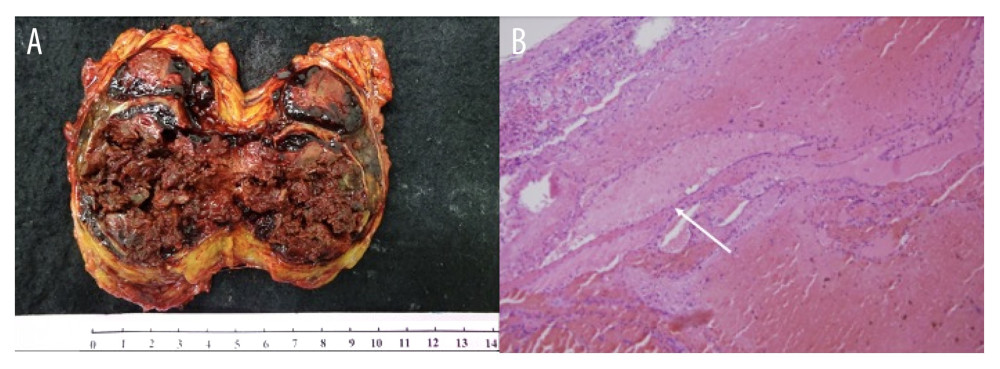
These tests revealed no evidence of hormonal hypersecretion. When the patient’s follow-up was resumed, ultrasound imaging revealed an enlarged suprarenal tumour. An MRI revealed a 64 cm tumour mass. The central part of the tumour resembled a hematoma, and dynamic contrast-enhanced images revealed progressive enhancement on the peripheral part. Because adrenal gland cancer was suspected, a laparoscopic adenectomy was performed. The surgical specimen revealed a brown-red tumour mass with a few blood clots on the surface, measuring 6.47.39 cm (Figure 3A). Histopathological examination revealed an adrenal endothelial (vascular) cyst with thrombi and calcification; the adrenal parenchyma was normal and free of malignancy.
Conclusions
Adrenal cystic lesions are uncommon and can range in histopathology from pseudocysts to malignant cystic tumours. With few cases reported and a wide range of differential diagnoses, the best way to treat adrenal cysts remains debatable.
Adrenal cystic lesions are rare and can range from benign cysts to cystic primary adrenal cancer. Although it is difficult to distinguish an adrenal cyst from other adrenal neoplasms, imaging studies such as CT and MRI are critical for defining an adrenal cystic lesion. Adrenal cysts can progress over time, so routine imaging during follow-up exams is recommended. An initial adrenal tumour evaluation should include an endocrine evaluation. It is important to consider the coexistence of functional neoplasms or functional cystic lesions. When the cyst is larger than 6 cm, malignancy is suspected, or abnormal endocrine activity is present, surgery is the first option.
Source: American Journal of Case Reports


