
- Giant ovarian cysts are a challenging condition in general practice because of the nonspecific clinical features. Physical examination includes a wide range of differential diagnoses.
- Giant ovarian cysts can cause serious complications, despite being asymptomatic, for example, perforation, obstruction, suppuration and torsion.
- The cysts often present with signs and symptoms of ascites because of their large nature and are often mistaken for it.
A 65-year-old female patient of African ethnicity presented with a 5-year history of chronic abdominal distention and was diagnosed with a giant ovarian cyst. She had no other gastrointestinal complaints, including abdominal pain, nausea and vomiting. However, she complained of an increase in urinary frequency. The patient was referred for management of massive ascites. She had a grand multiparity with parity of 6 (literature defines “grand multiparity” as a patient who has had more than 10 births, alive or stillborn at more than 20 weeks of gestation) and no other relevant past medical history.
On physical examination, pink conjunctivae and anicteric sclerae were seen. The patients weight was measured to be 65 kg and her vital parameters were normal. Abdominal examination showed that her abdomen was grossly distended with full flanks and visible striae. Similarly, the abdomen was also soft and non-tender with 115 cm of abdominal girth. Abdominal percussion was dull over the entire abdomen with presence of fluid thrill. There were no significant findings on examination of the cardiovascular and urogenital system.
Laboratory investigations revealed a normal complete blood count with a haemoglobin level of 12 g/dl. Ultrasound of the abdomen suggested a massive fluid-filled multiocular cavity originating from the right ovaries with a thin covering and bowel loops shifting against the diaphragm. Other test results, including the haematological or biochemical serum tests were normal.
The findings were consistent with the diagnosis of right multioculated ovarian cyst.
The patient was advised a right ovarian cystectomy via a laparotomy with a midline incision with counselling and consent.

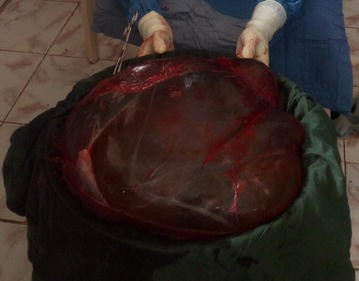
Intraoperative findings included a giant ovarian cyst originating from the right ovary with a gelatinous hyper vascularised membrane. The cyst was further excised with intact membranes, measuring 55 x 52 x 24 cm, weighing 10.8 kg.
Histopathological analysis showed a mucinous cystadenoma. The patient had an uneventful postoperative period and was discharged after 5 days of cyst removal with a weight of 54 kg.
References
Giant ovarian cyst masquerading as a massive ascites: a case report https://bmcresnotes.biomedcentral.com/articles/10.1186/s13104-017-3093-8


