
A 42-year-old woman, known case of multiple
sclerosis, rushed to the emergency department with complaints of accidental
foreign body insertion into her bladder during intermittent catheterization.
The patient had been performing
intermittent catheterization for the past 10 years as she had been suffering
from neurogenic bladder secondary to multiple sclerosis. This time the patient
stated that she accidentally pushed the catheter inside her urethra because she
confounded it with her vagina tampon.
Imaging:
An ultrasound was performed to confirm
the given history. On ultrasound, a foreign body was found inside the bladder
(Figure 1), which was coherent with her history.
Removal
of the foreign body:
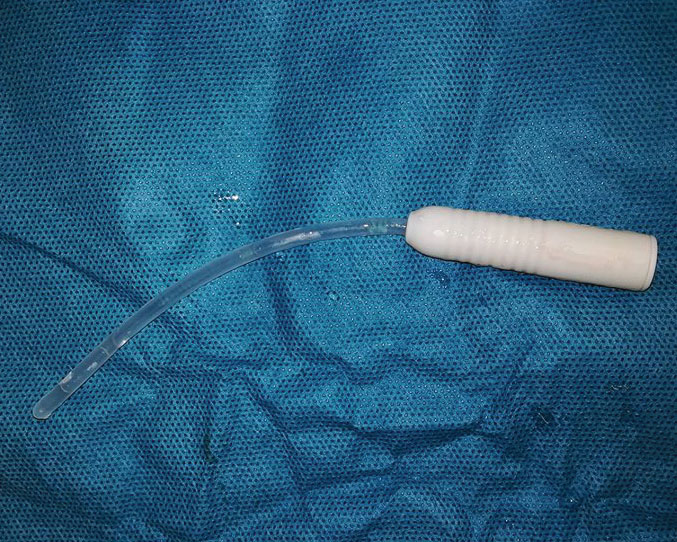
Cystoscopy was performed to remove the
foreign body. Under the cystoscopic direct vision, a 12Fr hydrophilic
single-use catheter was found, which was removed by grasping the tip and then
pulling it out through the urethra (Figure 2).
The patient suffered no complications, neither
due to the accidental misplacement of the catheter nor due to the extraction
procedure.
The female urethra, when compared
anatomically with the male urethra, provides an easier passage for the foreign
body to travel up the urethra as the female urethra is shorter and has no kink
or obstruction as seen in the male urethra due to the position of the prostate.
Most cases of the bladder foreign body
are related to sexual practices, including masturbation, sexual abuse, and
sexual fetish, or other psychiatric conditions.
Iatrogenic misplacement is also common. Rarely the patients present
themselves with a transurethral insertion, as seen in this patient.
Patients with intravesical foreign objects may present with lower urinary tract symptoms, including microscopic or gross hematuria, burning micturition, pain, irritation, and urinary tract infection. العاب القمار على الانترنت Asymptomatic and self-presentations are rarely seen. طريقة لعب بوكر Usually, due to fear or embarrassment, the patients present late or do not present until the symptoms are severe enough to seek medical attention. موقع مراهنات المباريات
Xrays can only detect radiopaque foreign
bodies, whereas, for all others,
ultrasound is necessary.
Usually, such patients are managed
endoscopically through the transurethral route. In cases where the patients
present late, the foreign body may encrust, hence necessitating open surgical
extraction. In male patients, careful removal is necessary to avoid erectile
dysfunction.
Since prompt and self-presentation is
rare, it is imperative to consider the foreign body in cases with chronic lower
urinary tract symptoms.
References:
Chondros K, Konsolakis I, Graikos K (2018) Young Woman with a Foreign Body into the Bladder. Clin Med Img Lib 4:125. doi.org/10.23937/2474-3682/1510125
Bansal A, Yadav P, Kumar M, et al. Foreign Bodies in the Urinary Bladder and Their Management: A Single-Centre Experience From North India. Int Neurourol J. 2016;20(3):260-269. DOI:10.5213/inj.1632524.262


