Case of ruptured endometrioma in a 32-year-old
Endometrioma is a type of ovarian cyst that occurs in 17-44% of endometriosis patients. They are caused by ectopic endometrial tissue haemorrhage within the ovary, resulting in degenerated blood products enveloped by ovarian parenchyma. Endometriomas are typically made up of fibrotic walls with a lining of endometrial epithelium, stroma, and glands. While they are frequently treated conservatively, complications such as rupture may necessitate surgical intervention. Rupture is most common in endometriomas larger than 6 cm in size and affects less than 3% of all known endometriomas. A ruptured endometrioma, on the other hand, can have serious consequences such as decreased fertility, adhesions, and pelvic pain.
According to current literature, ruptured endometriomas are rarely diagnosed preoperatively because they resemble other, more common abdominal emergencies. In these cases, ultrasound and cross-sectional imaging may be useful in identifying a ruptured endometrioma. A higher likelihood of a ruptured endometrioma will facilitate the decision to proceed with a laparoscopy. This article describes the case of a ruptured endometrioma that presented with clinical and imaging findings that raised the possibility of ovarian neoplasm. We hope to clarify some of the key findings that can help distinguish neoplasm from endometrioma before surgery.
Case study
A Hispanic woman, 32, presented with sharp pain in her upper to the mid abdomen. She had no significant medical history. But she complained of unexplained weight loss of 15 pounds over the previous 6 months. During the same time period, however, her abdomen grew in size. Her abdomen was distended at the time of admission, and a 3/6 systolic murmur was heard at the left upper sternal border. Leukocytosis to 17.5 103/MCL (normal 4.0-10.5 103/MCL), aspartate aminotransferase (AST) 273 U/L (normal 13-39 U/L), alanine transaminase (ALT) 149 U/L (normal 7-52 U/L), and cancer antigen-125 (CA-125) 4663 U/ML (normal 35 U/ML) were evident in the lab tests. Protein, ketones, and red blood cells were also detected in the urine.
Investigations and diagnosis
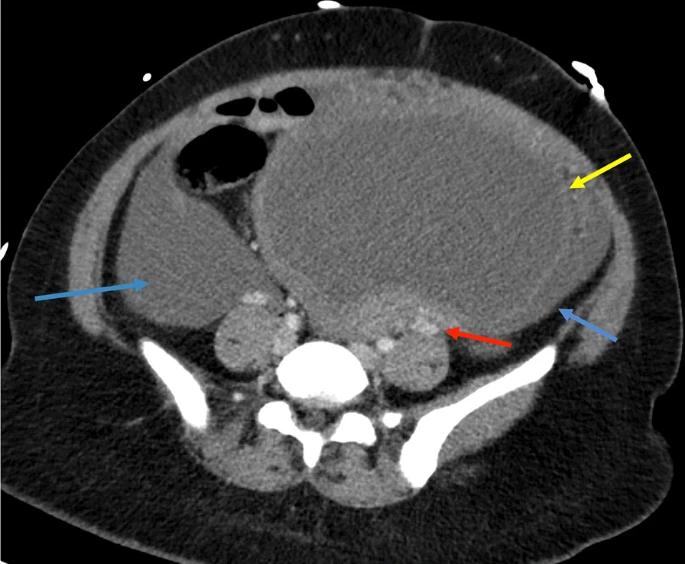
Doctors advised a contrast-enhanced computed tomography (CT) of the abdomen and pelvis which revealed a 13-cm complex cystic mass in the left adnexa with moderate hyperdense ascites and omental nodularity. The findings are consistent with the diagnosis of ovarian neoplasm with carcinomatosis. A large left adnexal complex cystic structure with internal echoes was revealed by pelvic ultrasound. A chest CT scan revealed no evidence of an intrathoracic neoplastic or infectious process. 700 mL of brownish opaque fluid was drained during diagnostic and therapeutic paracentesis and sent for culture and cytology, which later revealed benign histocytes and mesothelial cells.
Doctors further advised a diagnostic laparoscopy and tissue sampling by gynecologic oncology. An endometrioma with a thickened outer rind deeply adhered to the pelvic wall had completely replaced the left ovary. Superiorly, the cyst had a small ruptured area. Endometriosis deposits were found on the cyst, as well as the omentum and various peritoneal compartments sampled. A biopsy of the anterior abdominal wall was performed, revealing a minute fragment of fibrous tissue with a few pigmented macrophages and benign mesothelial cells.
Similarly, because this patient chose to not have any more children, doctors advised a radical hysterectomy with bilateral salpingo-oophorectomy, omentectomy, and peritoneal biopsies. Pathologic examination of the endometrium, myometrium, cervix, ovaries, fallopian tubes, peritoneum, omentum, and paracolic spaces revealed fibromuscular tissue with hemosiderin-laden macrophages and chronic inflammation, indicating the presence of multiple endometriosis foci. There were no hyperplastic, dysplastic, or malignant cells found in any of the samples.
Conclusion
In the absence of trauma, for premenopausal women with hemoperitoneum and complex adnexal cystic masses, endometrioma and the ruptured hemorrhagic cyst should be ruled out. In the case of a ruptured endometrioma, CA-125 and CA 19-9 levels can also be falsely elevated. Hence, as the study concludes, the possibility should be ruled out.
Source: Journal of Medical Case Reports


