- Frontoparietal abscess, also known as Pot’s Puffy tumour is a subperiosteal abscess that results from frontal sinusitis or trauma.
- The abscess associated with frontal bone osteomyelitis.
- Classic clinical presentation consists of frontal swelling, headache, fever and purulent rhinorrhea.
- Diagnosis can be confirmed with CT scan, whereas, treatment requires surgical intervention, analgesia and intravenous antibiotics.
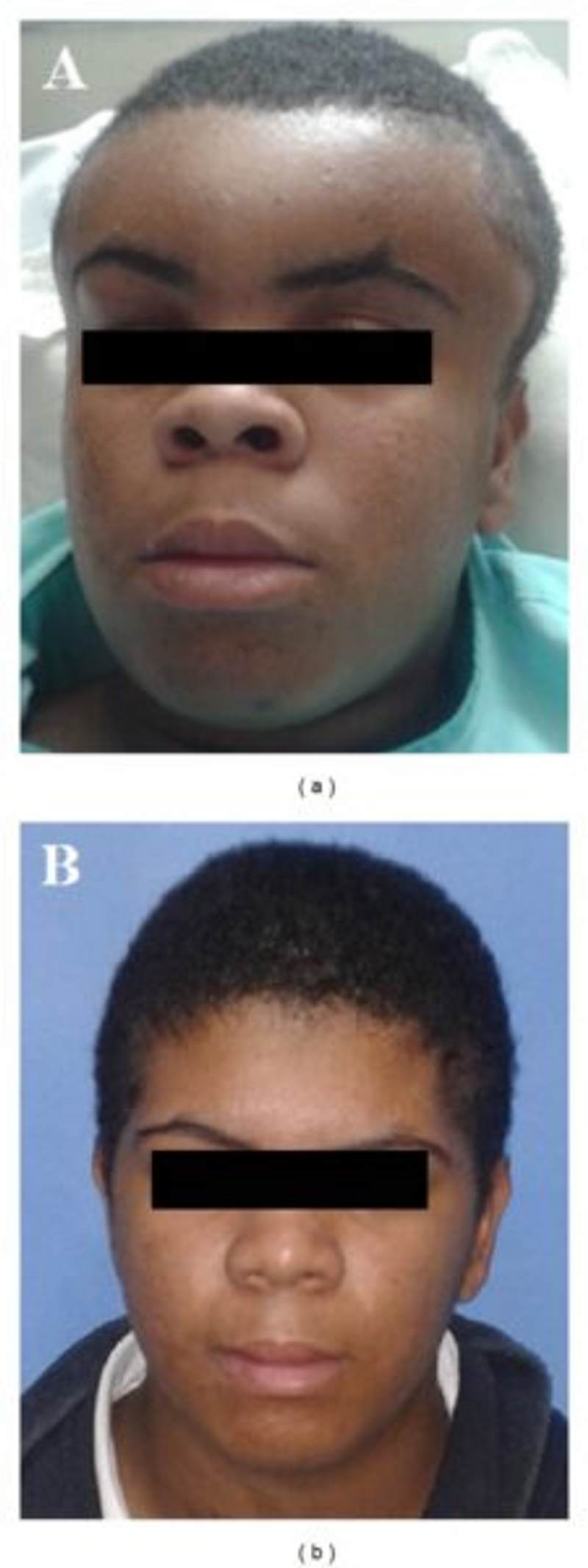
A 14-year-old male adolescent presented to the otorhinolaryngology department with a 7-day history of common cold with complaints of frontal headache, frontal and periorbital swelling, fever and vomiting. He had no significant past medical history. The adolescent had been hospitalised for 8 days earlier and was being treated with amoxicillin-clavulanate 3 g/day for seven days. There was only partial improvement of the periorbital oedema with no improvement in fever. Whereas, the frontal swelling worsened.
Physical examination showed signs of spontaneous purulent lacrimal discharge, periorbital oedema, painful and fluctuant swelling of the forehead and parietal region. Anterior rhinoscopy showed bilateral non-purulent discharge in common meatus, nonobstructive turbinates and hyperemic mucosa. Nasofibroscopy findings showed frontal recess purulent discharge which was greater on the left side. There were no signs of neurological abnormalities or systemic involvement. The remainder of the physical examination did not show any remarkable pathological changes.
A CT scan was performed to confirm the diagnosis which revealed soft tissue swelling of the forehead and parietal region, subcutaneous emphysema, opacification of the anterior ethmoid, maxillary and frontal sinus with erosion of the anterior table of the frontal sinus.
The treatment plan included surgical drainage of the abscess with combined approach (endoscopic endonasal and external drainage via coronal incision), in addition to an endoscopic intranasal frontal sinusotomy. Approximately 500 millilitres of thick purulent fluid was drained and sent for culture. Intraoperative inspection showed signs of necrosis of the temporal and frontal muscles associated with erosion of the external table of the frontal bone and osteomyelitis.
The patient remained in the intensive care unit for a few days. He recovered well with no remission of symptoms.
The culture was positive for Streptococcus constellatus, which is susceptible to multiple antibiotics. The 14-year-old was prescribed intravenous antibiotic therapy, metrondazole 2g/day for 5 days, vancomycin 2g/day and ceftazidime 6g/day for 18 days. However, metronidazole had to be exchanged for ampicillin-sulbactam because of suspicion of adverse reaction of drug.
The patient was discharged 25 days after the surgical drainage procedure. He presented with no complaints at follow-ups and normal physical examination.
References
Lauria, R. A., Laffitte Fernandes, F., Brito, T. P., Pereira, P. S. G., & Chone, C. T. (2014). Extensive frontoparietal abscess: complication of frontal sinusitis (Pott’s puffy tumor). Case reports in otolaryngology, 2014.


