
Such cases surprise the neurosurgeons. Cirsoid Aneurysm appears too rarely in population. There is no standard protocol for its treatment.
A young man, who reported some trauma to head around 8 years ago, presented with a slowly progressive swelling on the scalp. He noticed the swelling after the trauma. He had also undergone a surgery of the swelling around 2 years back but he had no documents. The swelling had been increasing gradually for last 8 years. Initially the swelling involved only parieto-occipital region but by the time he consulted medical help once again the swelling had extended towards the left fronto-temporo-parietal and occipital region. The scalp appeared irregularly bumpy! Apparently, the patient exhibited Parks Weber Syndrome but in scalp. Detailed examination presented a different diagnosis.
Upon examination the neurological status of patient was perfectly normal. Close examination of scalp presented irregular, soft, compressible, pulsatile scalp mass involving the whole left fronto-temporo-parietal and occipital region with large tortuous dilated vessels. Due to turbulent blood flow through the blood vessels audible bruit and palpable thrill were clearly noticeable.
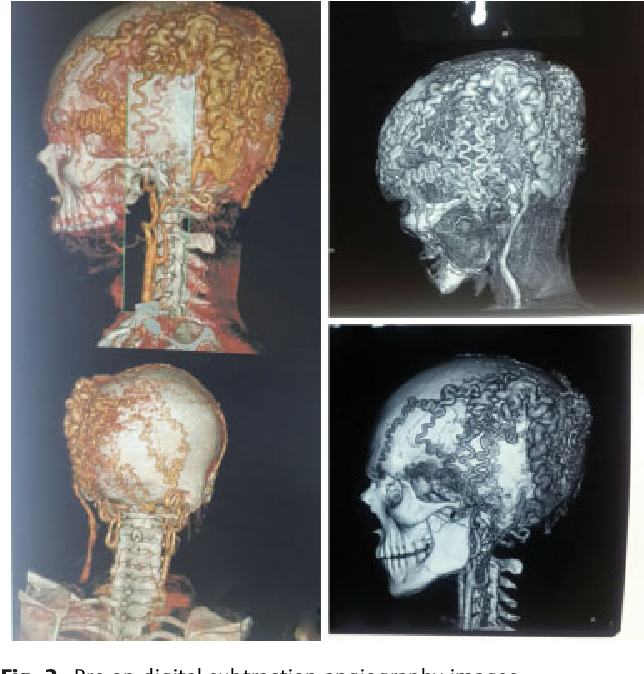
Digital Subtraction Angiography results
Digital Subtraction Angiography was performed to understand the status of condition accurately. This is the ideal and gold standard diagnostic test for aneurysms. They provide the imaging of excessive and abnormal links and connections of vessels. The results of angiography exposed complex left parietal scalp arteriovenous malformation. Left superficial temporal artery, left middle meningeal artery, and left occipital artery supplied this AVM with collateral supply from right superficial temporal artery and right occipital artery. Along the arteries there was equally complex venous contribution as well. Frontal, temporal and occipital scalp veins drained into external jugular vein. Digital Subtraction Angiography diagnosed the patient with Cirsoid Aneurysm. Due to the mesh-like network in the scalp the patient suffered from occasional headaches.
Although scalp has the most extensive and intense vascularity with high frequency of traumas yet the occurrence of Cirsoid Aneurysms are extremely rare. Their causes include congenital and traumatic interferences. Cirsoid Aneurysms are not life-threatening but continue being a risk for hemorrhage which leads to death. Initially the lesion appears in the form of small subcutaneous lump but evolves into large deforming mass. The presence of tortuous and pulsatile vessels on scalp produce social and cosmetics concerns for the patient.
En Block surgical excision
En block surgical excision is the most effective treatment approach in this case. This case of Cirsoid Aneurysm was quite complicated. therefore endovascular approach could not be opted and En block approach was preferred. Enblock is a French word which means ‘whole’. In this surgery, doctors removed the lesion in one unit without any divisions. Cutting through the lesion was not appropriate. After incising and devascularizing, the lesion was removed with pericranium, galea and temporalis muscle. Surprisingly, there was no loss of blood even though there was extensive network of vessels. During surgery, it was necessary to prevent any complication by having firm control over feeding arteries, carefully dissecting the scalp and removing pericranial component and temporalis muscle.
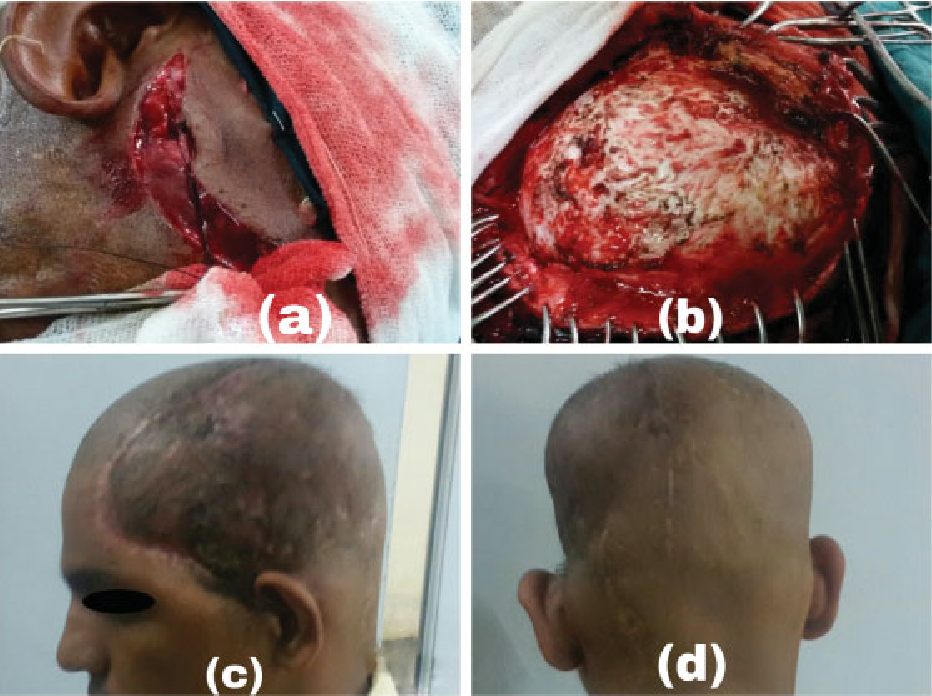
Postoperatively, a patch of necrotic scalp developed over a small area. No recurrence of AVM appeared upon conducting a CT scan. The patient was advised to continue follow-up.



