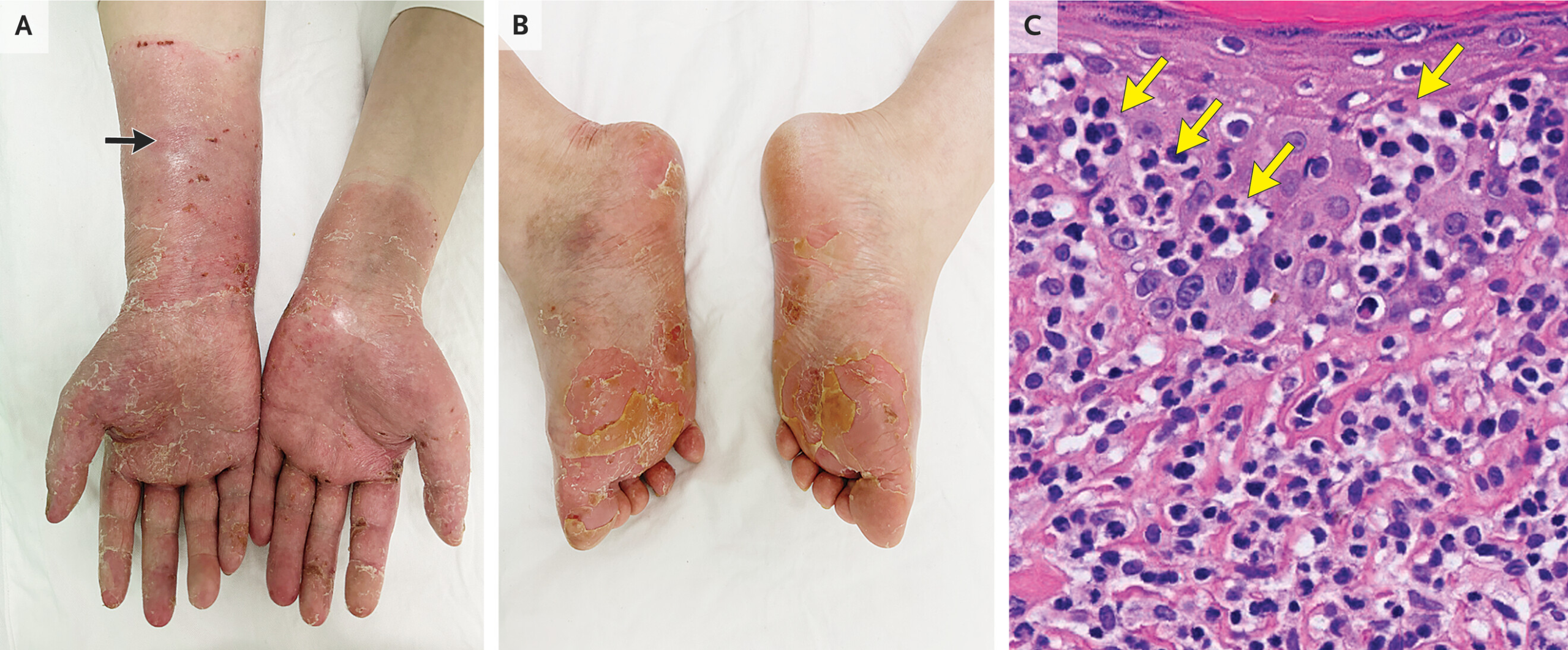
A 38-year-old man presented with a long-standing 15-year history of a recurrent rash involving both the palms and soles. The eruption was described as waxing and waning, with periods of partial improvement followed by recurrence. Over time, the lesions had become more persistent, prompting dermatologic evaluation. On examination, there were areas of erythematous to hyperpigmented patches with mild scaling on the palmar and plantar surfaces. To further investigate the underlying cause, a skin biopsy was performed, revealing dense lymphocytic infiltration of the superficial and mid-dermis.
This histopathological finding suggested a chronic inflammatory dermatosis rather than an acute infectious or allergic process. The combination of long disease duration, fluctuating course, and lymphocyte-predominant dermal inflammation narrowed the differential diagnosis to a small group of chronic papulosquamous or inflammatory skin conditions affecting acral sites.
One of the most important considerations in such a presentation is secondary syphilis, which is well known for its ability to mimic a wide range of dermatologic diseases. Secondary syphilis can present with a symmetrical rash involving the palms and soles, often appearing as reddish-brown macules, papules, or scaling plaques. The disease course is typically characterized by periods of improvement and recurrence if untreated, consistent with a waxing and waning pattern.
Histologically, secondary syphilis is classically associated with a dense dermal infiltrate composed predominantly of lymphocytes and plasma cells, often involving both the superficial and deep dermis. While plasma cells are a hallmark feature, lymphocyte-rich infiltrates are also commonly seen. This pattern reflects the host immune response to Treponema pallidum, the causative spirochete. The organism itself is often difficult to visualize on routine staining but may be detected using special techniques such as immunohistochemistry or dark-field microscopy.
Another important diagnostic consideration is chronic eczema or dermatitis, including dyshidrotic eczema or contact dermatitis affecting the hands and feet. These conditions can also present with recurrent flares and lymphocytic infiltration on biopsy. However, they are more commonly associated with spongiosis (intercellular edema of the epidermis), vesiculation, and a clear triggering exposure such as irritants or allergens. In contrast, the biopsy in this case demonstrated a predominantly dermal lymphocytic infiltrate without prominent epidermal spongiosis, making eczema less likely.
Psoriasis, particularly palmoplantar psoriasis, is another differential diagnosis. Psoriasis commonly affects the palms and soles and can have a chronic, relapsing course. However, histologically it is characterized by epidermal hyperplasia, parakeratosis, and neutrophilic microabscesses (Munro microabscesses), rather than a dense lymphocytic infiltrate in the dermis. The absence of these features makes psoriasis less consistent with the biopsy findings described.
Less commonly, conditions such as cutaneous T-cell lymphoma (mycosis fungoides) can present with chronic, relapsing skin lesions and a lymphocytic infiltrate. Early patch-stage mycosis fungoides may mimic eczema or psoriasis clinically and histologically. However, it typically shows atypical lymphocytes with epidermotropism (migration of lymphocytes into the epidermis) and sometimes Pautrier microabscesses. In this case, the biopsy description of a dense dermal infiltrate without mention of atypical lymphocytes or epidermotropism makes this diagnosis less likely but still worth excluding if clinical suspicion persists.
Given the strong clinical pattern of palmar and plantar involvement with a chronic relapsing course and lymphocyte-rich dermal inflammation, secondary syphilis remains a key diagnosis that must always be considered. Dermatologic manifestations of syphilis are often referred to as “the great imitator” because of their wide variability. Even in long-standing cases, lesions may persist or recur if infection remains untreated or inadequately treated.
Diagnosis of syphilis is confirmed through serologic testing, including non-treponemal tests such as RPR (Rapid Plasma Reagin) or VDRL, followed by confirmatory treponemal tests such as FTA-ABS or TPPA. In cases with atypical or long-standing presentations, these tests remain essential regardless of biopsy findings. Early recognition is critical because untreated syphilis can progress to systemic involvement, including neurological and cardiovascular complications.
Treatment of secondary syphilis is straightforward and highly effective. The standard therapy is intramuscular benzathine penicillin G, which leads to rapid resolution of lesions and prevents progression of disease. Alternative regimens are used in penicillin-allergic patients, depending on clinical circumstances. Importantly, even long-standing dermatologic manifestations can improve significantly after appropriate antimicrobial therapy.
This case highlights the importance of correlating clinical history with histopathological findings in chronic dermatologic disease. A long-standing, waxing and waning rash on the palms and soles with a dense lymphocytic dermal infiltrate should prompt consideration of systemic infectious causes, particularly syphilis, in addition to inflammatory and neoplastic conditions. Careful integration of clinical features, biopsy results, and serologic testing is essential for accurate diagnosis.
In summary, a chronic relapsing palmar and plantar rash with dense lymphocytic infiltration of the superficial and mid-dermis most strongly raises suspicion for secondary syphilis among other inflammatory dermatoses. Recognizing this pattern is crucial, as timely diagnosis and treatment can lead to complete resolution and prevent long-term complications.
Source: NEJM


