Case report
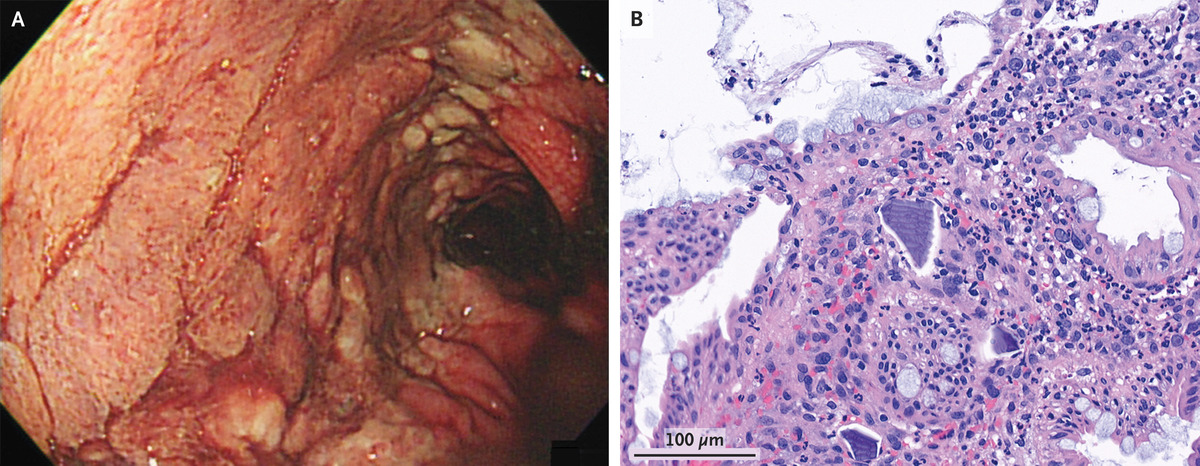
A 58-year-old woman was admitted to the hospital with a sudden onset bloody stools due to acute-on-chronic renal damage. She had hyperkalemia at the time of admission, and calcium polystyrene sulfonate — a cation-exchange resin that binds potassium in the colon — had been given many times per day for the first six days of her hospitalisation. On hospital day 6, a huge volume of painless hematochezia emerged, as did a significant fall in haemoglobin level. A continuous ulcer extending from the splenic flexure to the rectum was discovered during a colonoscopy (Panel A). There was no evidence of active bleeding. This article highlights the case of calcium polystyrene sulfonate-induced colonic necrosis and perforation.
In a necroinflammatory setting, a sample of the intestinal mucosa revealed epithelial damage and basophilic calcium polystyrene sulfonate crystals (Panel B). Calcium polystyrene sulfonate-related colonic necrosis was diagnosed. In rare situations, calcium polystyrene sulfonate or its equivalent, sodium polystyrene sulfonate, can cause gastrointestinal damage. The precise frequency and mechanism are unknown. The colon is the most commonly affected location. The patient’s hematochezia improved once the culprit medication was discontinued and bowel rest was implemented. On hospital day 45, she was discharged with better renal function and a normal potassium level. Colonic necrosis has been noted as a rare consequence following Kayexalate use. We present a case of calcium polystyrene sulfonate-induced colonic necrosis and perforation in this case study to warn practitioners of this uncommon but deadly complication linked with this regularly used medicine.
Colonic necrosis and perforation due to calcium polystyrene sulfonate
The ion-exchange resin sodium or calcium polystyrene sulfonate (Kayexalate or analogue) is extensively used to treat hyperkalaemia in individuals with chronic renal disease. It has been linked to digestive issues such as nausea, vomiting, and constipation. Although uncommon, colonic necrosis and perforation are serious side effects of the medicine. Calcium polystyrene sulfonate-induced colonic necrosis and perforation is highlighted in this case report to warn practitioners of this uncommon but dangerous complication linked with this frequently administered medicine.
Sodium polystyrene sulfonate can also bind intraluminal calcium, which can cause constipation, faecal impaction, and intestinal obstruction or perforation. The true incidence of colonic necrosis with Kayexalate is unknown. Gerstman et al. observed a 0.27% overall incidence, with a higher postoperative incidence (1.8%). Lillemoe et al. first described colonic necrosis caused by Kayexalate-sorbitol enemas, along with experimental proof that the necrosis was caused by sorbitol rather than Kayexalate in the presence of uraemia. In all the uraemic and non-uraemic groups, rats given sorbitol or Kayexalate in sorbitol enemas had extensive transmural necrosis.
In this case, it is uncertain what caused the necrosis or the perforation
It is uncertain what caused the necrosis and perforation. Elevated renin levels, which are prevalent in renal insufficiency, may predispose the patient to non-occlusive mesenteric ischaemia by angiotensin-mediated vasoconstriction. One gramme of Kayexalate has a theoretical in vitro potassium exchange capacity of 2-3.1 mEq and an in vivo capacity of 1 mEq. According to Emmett et al., in vivo potassium-binding capacity may be lower than previously predicted, ranging from 0.4 to 0.8 mEq/g of Kayexalate resin. Colonic perforation, in contrast to other mild digestive problems associated with Kayexalate therapy, causes considerable morbidity and mortality.
As a result, potassium exchange resins may, though infrequently, cause a colonic perforation, and this diagnosis should be investigated in a patient treated for acute abdomen. Clinicians must be aware of the infrequent but serious problems associated with potassium exchange resins.
Source: NEJM


