Atopic eruption of pregnancy in a 37-year-old primigravid woman
Pregnancy skin changes can be physiological (hormonal), changes in pre-existing skin diseases, or the development of new pregnancy-specific dermatoses. Pregnancy-specific skin dermatoses are a diverse group of pruritic skin eruptions that occur only during pregnancy. These include atopic pregnancy eruption, polymorphic pregnancy eruption, pemphigoid gestationis, and pregnancy intrahepatic cholestasis. The most common of these disorders is atopic eruption of pregnancy. Most postpartum skin eruptions resolve on their own and only require symptomatic treatment. Patients with pemphigoid gestationis and intrahepatic cholestasis of pregnancy should be monitored antepartum because they pose a foetal risk. This article discusses the classification, clinical features, and treatment of pregnancy-related dermatoses.
Vaughan-Jones et al. reported a high prevalence of atopic eczema in pregnancy for the first time in a prospective study on pruritic skin diseases in pregnancy in 1999. This finding contradicted previous classifications, which concluded polymorphic eruption of pregnancy as the most common dermatosis in pregnancy. The increased incidence of atopic eczema in pregnancy has been attributed to immunological changes during pregnancy. To prevent foetal rejection, pregnancy is characterised by a lack of strong maternal cell-mediated immune function and T-helper 1 (Th1) cytokine production (eg, IL-12, interferon gamma) and a dominant humoral immune response and T-helper 2 (Th2) cytokine production (eg, IL-4, IL-10). 5 The Th2 shift associated with pregnancy may favour atopic dermatitis exacerbation.
Case study
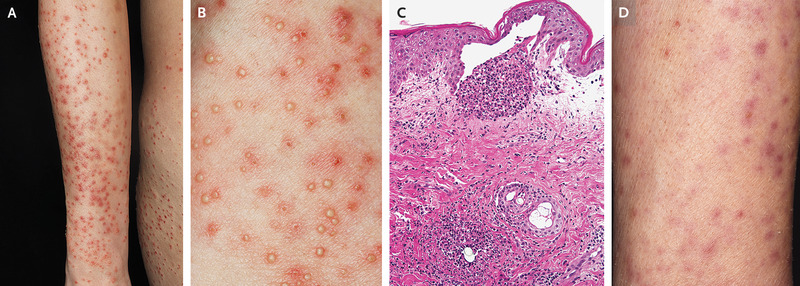
At 30 weeks’ gestation, a 37-year-old primigravid woman presented to the dermatology clinic with a 4-month history of pruritic pustules on her torso, arms, and legs. On examination, papules, nodules, and follicular pustules with surrounding erythema were found on the trunk, arms, and legs, but no lesions were found on the palms and soles (Panel A shows the left arm, and Panel B a closer view of the left arm). The lesions did not improve despite the use of topical and oral glucocorticoids to treat a possible diagnosis of polymorphic eruption of pregnancy. A skin biopsy was performed on the day of the initial presentation, revealing subepidermal pustules and perifollicular neutrophilic infiltration (Panel C, hematoxylin and eosin staining).
Diagnosis and treatment
Gram’s, periodic acid-Schiff, and Grocott methenamine silver stains all came back negative. Atopic eruption of pregnancy was diagnosed. The most common dermatosis of pregnancy is atopic eruption. Eczema, prurigo, and, as seen in this case, pruritic folliculitis are all examples. Atopic pregnancy eruption is typically associated with a history of atopy, which this patient lacked. The condition poses no danger to the foetus. Cyclosporine and a higher dose of oral glucocorticoid were prescribed due to the patient’s severe pruritus. The lesions had subsided after two weeks of observation (Panel D shows the left arm).
Atopic eruption of pregnancy and polymorphic eruption of pregnancy are benign skin conditions and do not carry any fetal risk. They usually resolve in the early postpartum period. During pregnancy, they respond well to topical emollients and moderately potent steroids in combination with oral antihistamines. Systemic steroids may be used for severe cases of PUPPP. Pruritic folliculitis responds well to topical benzoyl peroxide and also has been treated with narrowband (TL-01) ultraviolet B phototherapy. Patients with pemphigoid gestationis and intrahepatic cholestasis of pregnancy carry fetal risk and require specific treatment. Mild pruritus can be treated with oral antihistamines but patients with more severe cases of PG require systemic corticosteroids. immunoglobulins.
High-dose intravenous immunoglobulins have also been used to treat PG. Ursodeoxycholic acid is the drug of choice for ICH because it is the only therapy that has been shown to reduce both maternal pruritus and foetal mortality.
Source: NEJM


