
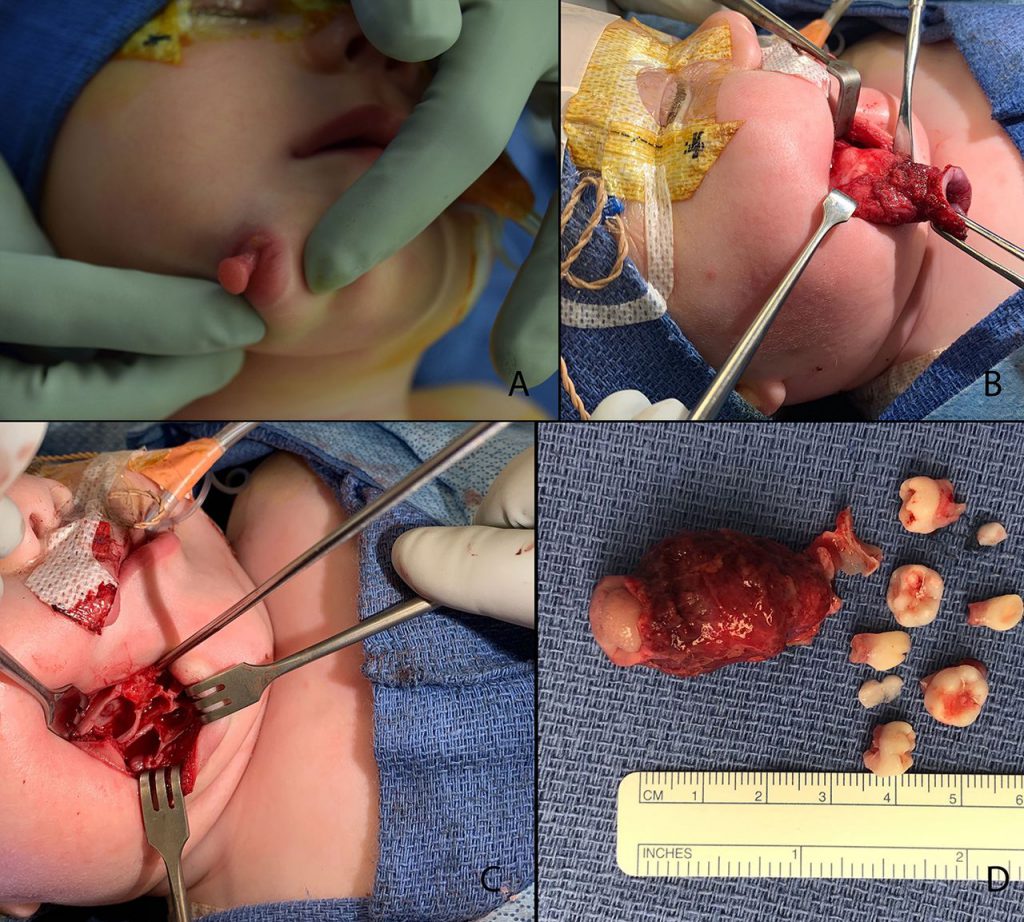
Doctors at South Carolina Medical university were left stunned by an extremely rare birth defect in a newborn baby girl who was born with not one but two mouths. The duplicated oral cavity was seen to have its own lip, 6 teeth, and a primitive tongue that moved in sync with the tongue in her main mouth.
Source: Hamberis et al., BMJ Case Reports, 2020
According to the case report published in BMJ Journals, the defect was first noted as a right mandibular mass on a prenatal ultrasound scan in the third trimester of the pregnancy. Doctors initially gave a differential diagnosis of a cyst or sinus, teratoma, fibrous dysplasia, or foregut duplication. There was no family history of facial malformations and the mother denied any exposure to teratogens. The baby was born at 40 weeks by an uncomplicated vaginal delivery.
On examination, no signs of respiratory compromise were seen. An inability to depress the right lower lip was present in the newborn, however, the rest of the head and neck examination was unremarkable.

Source: Hamberis et al., BMJ Case Reports, 2020
MRI and, later a CT scan done at 2 weeks of age, confirmed the presence of a partially ossified soft tissue mass containing several unerupted teeth. A follow-up appointment at two weeks showed the infant to be healthy and feeding well. The second oral cavity was not seen to be in communication with the main oral community and the airway was not compromised.
Diprosopus is the name given to duplications of craniofacial structures which can range from complete facial duplication to partial duplication of facial structures. It is an extremely rare condition with only 35 cases recorded since the 1900s. Despite its rarity, these duplications are associated with a risk that the structures could communicate with the oral cavity and involve the airway, compromising the patient’s airway and/or feeding. Therefore, at the time of delivery, it is important for an otolaryngology team to be present and the airway to be secured. These duplications are usually diagnosed in-utero or shortly after birth.
Surgical intervention of duplications involving the mandible should be deferred until the accessory teeth can be distinguished on imaging, as premature resection can cause unintentional damage to the unerupted permanent teeth.
Source: Hamberis et al., BMJ Case Reports, 2020
While studies suggest that this particular anomaly occurred due to duplication of the first branchial arch, authors of this study argue this could not have been the case as all other first branchial arch derivatives in the infant were normal. The baby’s inability to depress the lower lip was considered a nerve defect and believed to be due to second arch disruption.

Source: Hamberis et al., BMJ Case Reports, 2020
At 6 months of age, the infant underwent surgery for excision of the duplicated structure, bony contouring of the mandible, and closure of the soft-tissue defect with adjacent tissue transfer. The Post-op pathology report showed the mass contained salivary gland, skeletal muscle, and dental pulp with six benign molar teeth. At her 6-month follow-up, apart from an inability to depress the right lower lip, the baby was seen to be healing well and feeding without difficulty.
References:
Hamberis AO, Macias D, Clemmens C, et al. Duplication of the oral cavity and mandible: a rare congenital craniofacial anomaly. BMJ Case Reports CP 2020;13:e233799.
Mews L, Isaac A, Leonard N, et al. A duplication of the mouth associated with a dysontogenic cyst: a case report and discussion of theories of origin. JAMA Otolaryngol Head Neck Surg 2014;140:464–8


